
Clubfoot Awareness Week
Clubfoot Awareness Week
June, 3 2020
This week (1st to 7th June 2020) is Clubfoot Awareness Week and we thought what better time to talk about the signs and symptoms to look out for that may indicate an underlying problem.

Every day 500 babies are born worldwide with a condition called Congenital Talipes Equino Varus, commonly known as Clubfoot or Talipes. Club foot is quite common, affecting about 1 baby in every 1,000 born in the UK and both feet are affected in about half of these babies. It is twice as common in boys than girls.
The majority of babies born with clubfoot live in lower and middle income countries and unfortunately cannot access treatment. Those children who do not access treatment face a lifetime severely affected by clubfoot, experiencing ongoing pain, limited mobility, and reduced opportunities in education, employment and relationships.
Until relatively recently in certain countries, children that were able to access healthcare were treated with major surgery. The results from surgery were often ineffective. Increasingly more and more evidence indicates that the longer term impact of cases that were initially considered successful outcomes were also poor, leaving the feet of patients stiff and painful over time.
World Clubfoot Day takes place on 3 June and this marks the Birthday of Dr Ignacio Ponseti – the pioneer of a global, minimally invasive and successful treatment for Talipes/Clubfoot.
What is Clubfoot?
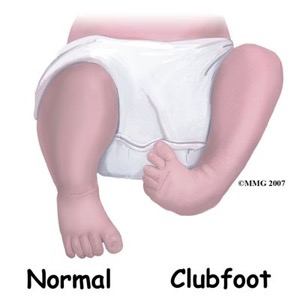
Clubfoot refers to a condition in which a newborn’s foot or feet appear to be rotated internally at the ankle. The foot points down and inwards, and the soles of the feet face each other. It is known as talipes equinovarus (TEV) or congenital talipes equinovarus (CTEV). In 50 percent of cases, both feet are affected. Although sounding complicated, when broken up, it becomes easier to understand.
- Congenital – Present at birth
- Talipes – the foot and ankle
- Equino – foot pointing down
- Varus – heel turning inwards
In clubfoot, the tendons on the inside of the leg are shortened, the bones have an unusual shape, and the Achilles tendon is tightened. If left untreated, the person may appear to walk on their ankles or the sides of their feet.
Club foot isn’t painful for babies, but if it isn’t treated, it can become painful and make it difficult to walk as they get older.
Clubfoot can be classified into 4 categories:
Congenital clubfoot is by far the most common, and most affected children have no other conditions. It is sometimes referred to as isolated clubfoot or idiopathic (meaning cause unknown) clubfoot. Idiopathic clubfoot occurs in about 1 to 2 per 1000 live births.
Positional clubfoot occurs when an otherwise normal foot is held in an incorrect position in the womb (as seen in the picture below). The foot is flexible rather than rigid and can be manipulated into a neutral position easily by hand. Physiotherapy usually corrects this type of clubfoot.

Complex or Atypical clubfoot refers to feet which are more resistant to routine treatment but are still correctable, using a slightly different casting technique. Atypical feet are short and chubby with a deep crease across the sole. The big toe may also stick up at an odd angle to the other toes.
Syndromic clubfoot, which occurs in only a small minority of cases, is associated with additional chromosomal/ genetic abnormalities or syndromes. Further tests may be offered to you by your consultant.
Causes of clubfoot
In most cases the cause of clubfoot isn’t known (idiopathic), but there may be a genetic link as it can run in families.
If you have one child with clubfoot, your chance of having a second child with the condition is about 1 in 35. If one parent has club foot, there’s about a 1 in 30 chance of your baby having it. If both parents have the condition, this increases to about a 1 in 3 chance. In rare cases, club foot can be linked to more serious conditions, such as spina bifida or a developmental hip condition known as hip dysplasia, or developmental dysplasia of the hip (DHH).
Diagnosing clubfoot
Club foot is usually diagnosed after a baby is born, although it may be spotted in pregnancy during the routine ultrasound scan carried out between 18 and 21 weeks. Club foot can’t be treated before birth, but picking up the problem during pregnancy means you can talk to doctors and find out what to expect after your baby is born.
Treating clubfoot
A clubfoot will not improve without treatment and leaving the foot untreated increases the risk of complications later in life.
Treatment for clubfoot usually starts within a week or two of your baby being born. A technique known as the Ponseti method is the main treatment for clubfoot nowadays. This involves gently manipulating your baby’s foot into a better position, then putting it into a cast from the toes to the thigh, to hold the foot in position. This is repeated every week for about 5 to 8 weeks. The manipulation and casting are done very gently, and your baby should experience no pain.

After the last cast comes off, most babies need a minor operation known as a tenotomy to loosen the tendon at the back of their ankle (Achilles tendon). This is done using a local anaesthetic. It helps to release their foot into a more natural position.
Once the foot is corrected your baby will need to wear special boots attached to each other with a bar to prevent the club foot returning. The boots are worn for 23 hours a day for the first 3 months and then just at night and nap times for up to the age of 4 or 5 years old. Regular footwear may then be worn at all other times.

For the Ponseti method to be effective, it has to be done very early on, and parents have to make sure the boots are worn according to instructions. If instructions are not followed strictly, the foot may return to its original position, and treatment has to start again. While the infant is wearing a cast, parents should monitor for changes in skin color or temperature, as this could mean that the cast is too tight.
Steps have produced a great booklet for parents about talipes and its treatment https://www.steps-charity.org.uk/wp-content/uploads/2020/03/Talipes_Clubfoot.pdf
Surgery
Surgery may be used if other methods do not work, but this is normally on a case-by-case basis. Surgery aims to adjust the tendons, ligaments, and joints in the foot and ankle, for example, by releasing the Achilles tendon or by moving the tendon that goes from the front of the ankle to the inside of the foot.
More invasive surgery releases soft tissue structures in the foot. The surgeon then stabilizes the foot using pins and a cast. Surgery is always used as a last resort as it may lead to overcorrection, stiffness, and pain. It has also been associated with arthritis later in life.
Outlook
Nearly all children treated with the Ponseti method will have pain-free, normal-looking feet.
Most learn to walk at the usual age and can enjoy physical activities, including sports when they’re older.
Even with treatment, children who only have one affected foot may be left with a slightly shorter leg and smaller foot on one side (between one and one-and-a-half times smaller than the other foot, and slightly less mobile). The calf of the leg will also be smaller and this may mean your child is slightly less mobile and gets tired more quickly than other children.
Relapses
A well-treated clubfoot should not leave a child at a disadvantage. They will be able to run and play like other children. Sometimes clubfoot can come back, especially if treatment isn’t followed exactly. If it comes back, some of the treatment stages may need to be repeated. Left untreated, however, complications can occur and before the Ponseti method, club foot was often treated with surgery to alter the position of the foot. This wasn’t always effective, and led to long-term pain and stiffness for some adults.
How can physiotherapy help my child?
Here at The Children’s Physio we are highly specialised in assessing and treating children with a wide variety of conditions from babies through to adolescents. Our paediatric physiotherapists have the expertise and clinical training to provide early treatment to children with symptoms of Clubfoot. We will provide a comfortable assessment of your child and ensure the highest level of care at all stages of treatment.
What should be expected from Physiotherapy treatment?
Physiotherapy after surgery for a clubfoot can begin as soon as your child’s surgeon recommends it. All treatment, either surgical or non-surgical including physiotherapy, is designed to give the child a foot that can be placed flat on the floor. Another goal of Physiotherapy is to assist your child’s walking biomechanics in order to encourage your child to walk as efficiently as possible. Lastly, our goals also include relieving any pain if present, preventing pain in the future, maintaining the flexibility of your child’s muscles and tissues, and preventing any weaknesses around the lower extremities and core from developing.
- Depending on the age of your child, once the brace is discarded during the day, your physiotherapist may incorporate taping techniques of the foot to provide gentle foot positioning guidance.
- Your physiotherapist may address any pain issues that your child may be experiencing from the surgical procedure or the deformity itself, depending on the age of your child. Your physiotherapist may use modalities such as ice, heat or massage to try to relieve any pain.
- Maintaining the length of the tissues in your child’s foot is the main goal of any stretching exercises we do with your child or ask you to do with them.
Your child’s age at the time of surgery will largely influence how formal the stretches and strengthening exercises for your child will be.
Stretches
If your child is old enough to understand and follow along, your physiotherapist may encourage specific stretches for the back of the calf and Achilles tendon, as well as for the bottom of the foot.
Often, however, children who have had surgery for clubfoot are too young to effectively engage in formal stretches therefore play activities that encourage these types of stretches will be taught. Ensuring that your child spends time squatting, standing with feet flat, standing on their toes, standing on their heels, walking without the brace, and practicing jumping are ways to encourage proper foot movement. Your physiotherapist will guide you through which of the activities are most important for your child at which time, the proper technique for these activities, and how long they should be performing each activity.
If your child is too young to walk or do the higher level activities then your physiotherapist will teach you age-appropriate play activities that encourage the proper positioning of your child’s foot and lower leg. Range of movement exercises that encourage motion of the foot in all directions away from the clubfoot position will be important. Of particular importance are passive Achilles tendon stretches, which will be taught to you and will be encouraged frequently. The Achilles tendon is the thick tendon at the back of the ankle.
Strengthening
Formal strengthening exercises for older children will be taught which encourage ankle, calf, hip, and core strengthening as well strengthening for the muscles that pull the foot into a position where the sole of the foot is turned up and out (opposite to the clubbed foot position). As previously mentioned often the child who has had surgery for clubfoot is too young to perform any formal exercises. Playing is once again the best method to encourage strength development in your child’s feet, legs and core area.
Your physiotherapist will encourage fun play activities and games such as assisted frog jumps or hops on one leg in order to strengthen the appropriate muscles. Even helping the young child mimic these types of activities can be very useful to strengthen the legs and feet and encourage proper foot position. Any activity they enjoy which encourages the proper motion is useful! Often singing while doing activities or making a game of the exercises is the best method of incorporating rehabilitation into your young child’s world.
For those children that are old enough to ambulate, gait retraining when the brace is off is a crucial part of rehabilitation after surgery for clubfoot. Your physiotherapist will also work on your child’s foot and ankle proprioception (knowing where their foot is in space without them having to look at it) by having them stand or walk on different surfaces such as a soft mat or foam, as well as on different angles. Activities such as hopping or climbing on apparatus will also help to improve their proprioception. Climbing up onto things such as stairs or gym equipment simultaneously helps to build the needed strength in the hip area, which is an important area that assists in controlling the knee and foot position.
For children who are not yet walking, holding them in the standing position (with proper foot alignment) on different surfaces as well as on different angles will accomplish the same thing. Most importantly, for all exercises, the goal is to get the foot into a proper weight bearing position and keep it out of the clubbed foot position.
Your physiotherapist will be a useful resource for discussing footwear modifications for your child if needed. They may consult with a Podiatrist or Orthotist to ensure that the most appropriate footwear is prescribed for your child.
As your child grows, rehabilitation will need to be continued but the frequency of sessions should decrease as long as early intervention has started your child on the right path to correcting the alignment of your child’s foot, ankle, and lower limb, and as long as you are actively doing the home rehabilitation program. As your child grows and becomes more mature, physiotherapy will include more formal types of exercises to encourage proper foot alignment. It is expected that your child will eventually be able to partake in all physical activities that other children their age partake in.
Generally children who have had surgery for clubfoot do extremely well with the physiotherapy we provide at The Children’s Physio. Over the course of your child’s therapy your physiotherapist will liaise closely with your child’s doctor, surgeon, orthotist or podiatrist as well as any other health care professionals that are involved in their care to ensure your child is recovering as quickly and normally as possible.
Remember, if you have any questions or concerns relating to your childs’ feet or their general development The Children’s Physio will be able to advise. You can find us at https://thechildrensphysio.com.
More support for club foot
The charity STEPS offers help and support for families of children with clubfoot, and also adults who were born with clubfoot. You can call their helpline on 01925 750271 or email info@steps-charity.org.uk.
Information about your child
If your child has club foot, your clinical team will pass information about him or her on to the National Congenital Anomaly and Rare Diseases Registration Service (NCARDRS). This helps scientists look for better ways to prevent and treat this condition. You can opt out of the register at any time.